Theory of pharmacology
This section needs expansion. You can help by adding to it. (July 2019) |
The study of chemicals requires intimate knowledge of the biological system affected. With the knowledge of cell biology and biochemistry increasing, the field of pharmacology has also changed substantially. It has become possible, through molecular analysis of receptors, to design chemicals that act on specific cellular signaling or metabolic pathways by affecting sites directly on cell-surface receptors (which modulate and mediate cellular signaling pathways controlling cellular function).
Chemicals can have pharmacologically relevant properties and effects. Pharmacokinetics describes the effect of the body on the chemical (e.g. half-life and volume of distribution), and pharmacodynamics describes the chemical's effect on the body (desired or toxic).
Systems, receptors and ligandsedit
This section needs expansion. You can help by adding to it. (July 2019) |
Pharmacology is typically studied with respect to particular systems, for example endogenous neurotransmitter systems. The major systems studied in pharmacology can be categorised by their ligands and include acetylcholine, adrenaline, glutamate, GABA, dopamine, histamine, serotonin, cannabinoid and opioid.
Molecular targets in pharmacology include receptors, enzymes and membrane transport proteins. Enzymes can be targeted with enzyme inhibitors. Receptors are typically categorised based on structure and function. Major receptor types studied in pharmacology include G protein coupled receptors, ligand gated ion channels and receptor tyrosine kinases.
Pharmacologyedit
This section needs expansion. You can help by adding to it. (July 2019) |
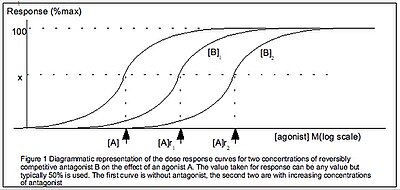
Pharmacodynamics is defined as how the body reacts to the drugs. Pharmacology models include the Hill equation, Cheng-Prusoff equation and Schild regression. Pharmacodynamics theory often investigates the binding affinity of ligands to their receptors.
Medication is said to have a narrow or wide therapeutic index, certain safety factor or therapeutic window. This describes the ratio of desired effect to toxic effect. A compound with a narrow therapeutic index (close to one) exerts its desired effect at a dose close to its toxic dose. A compound with a wide therapeutic index (greater than five) exerts its desired effect at a dose substantially below its toxic dose. Those with a narrow margin are more difficult to dose and administer, and may require therapeutic drug monitoring (examples are warfarin, some antiepileptics, aminoglycoside antibiotics). Most anti-cancer drugs have a narrow therapeutic margin: toxic side-effects are almost always encountered at doses used to kill tumors.
The effect of drugs can be described with Loewe additivity.clarification needed
Pharmacokineticsedit
This section has multiple issues. Please help improve it or discuss these issues on the talk page. (Learn how and when to remove these template messages)
(Learn how and when to remove this template message)
|
Pharmacokinetics is the study of the bodily absorption, distribution, metabolism, and excretion of drugs.
When describing the pharmacokinetic properties of the chemical that is the active ingredient or active pharmaceutical ingredient (API), pharmacologists are often interested in L-ADME:
- Liberation – How is the API disintegrated (for solid oral forms (breaking down into smaller particles), dispersed, or dissolved from the medication?
- Absorption – How is the API absorbed (through the skin, the intestine, the oral mucosa)?
- Distribution – How does the API spread through the organism?
- Metabolism – Is the API converted chemically inside the body, and into which substances. Are these active (as well)? Could they be toxic?
- Excretion – How is the API excreted (through the bile, urine, breath, skin)?
Drug metabolism is assessed in pharmacokinetics and is important in drug research and prescribing.

Comments
Post a Comment